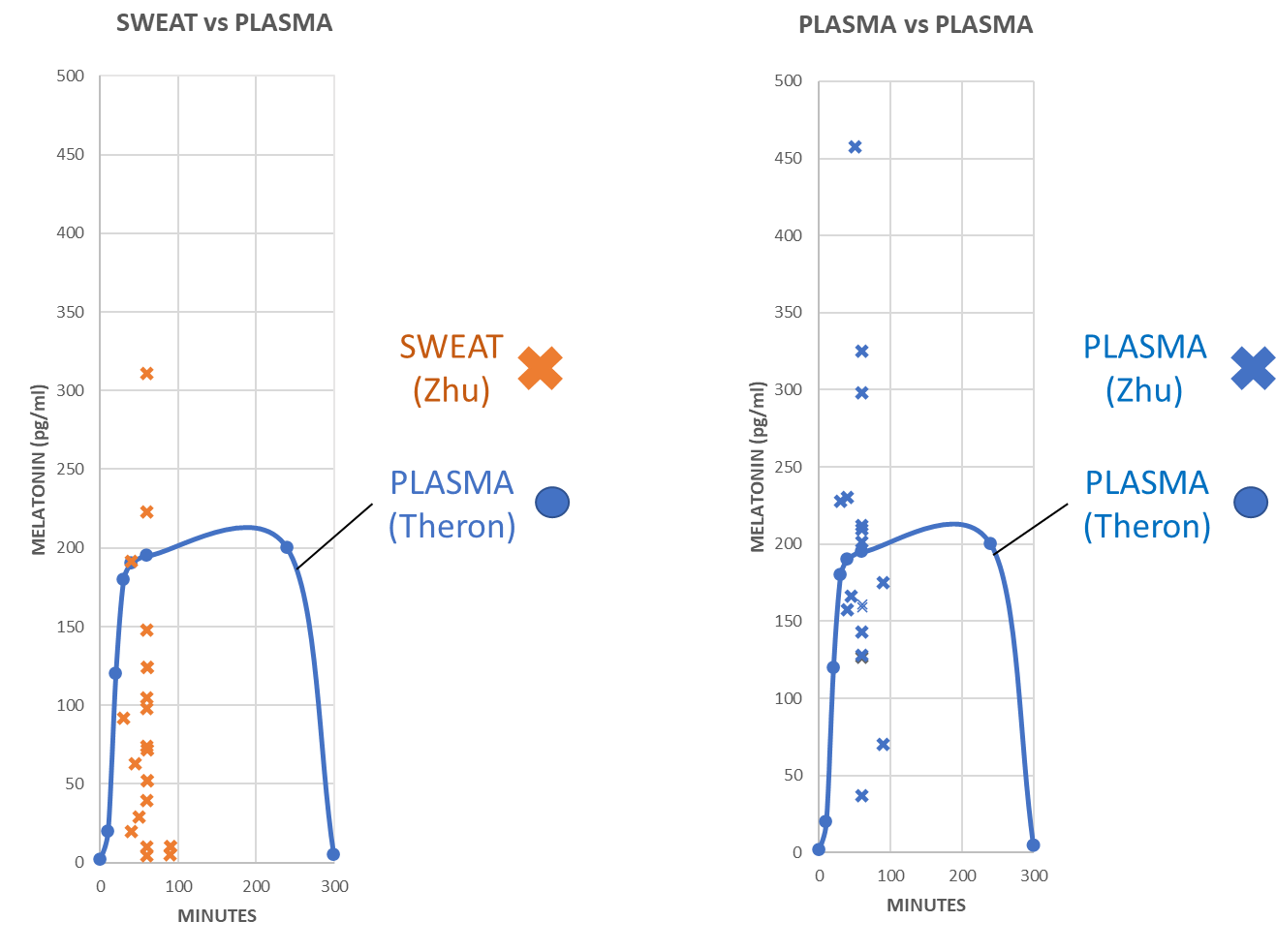
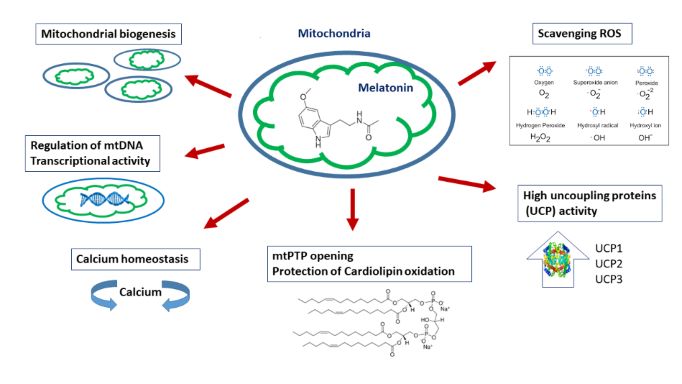
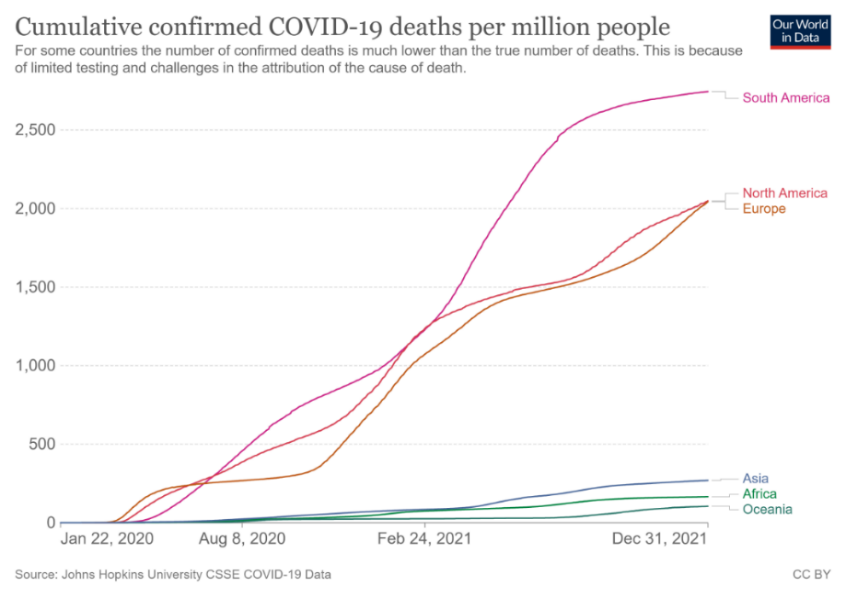
One of the most interesting and thought-stimulating papers in the current issue is the report published by Skutsch et al.; they noted that COVID-19 deaths per million were higher in South America than in either Europe and North America, while Asia, Africa, and Oceania had death rates which were only a fifth of those in South America. They found that the COVID-19 death rate was strongly associated with overweight and high latitudes but not with the vaccine coverage percentage in these countries. In an attempt to explain these differences, they hypothesized that: (1) In overweight people there is less penetration of near-infrared radiation (NIR) to the depth of important organs; stimulation of these organs by NIR would result in elevated production of subcellular melatonin, a strong antioxidizing factor. (2) In overweight people, fatty tissue holds much of the body´s 25(OH)D3 leaving less circulating in the blood making it less systemically protective. The hypothesis advanced by Skutsch et al. receives support from an article by Zimmerman and Reiter published also in this issue. They observed that large quantities of melatonin, greater than 5 pg/ml min ramp rates for plasma and sweat melatonin in human subjects, have been detected during strenuous exercise in sunlight as compared to 0.15 pg/ml min ramp rates for plasma melatonin under dim light melatonin onset conditions. This difference is in excessive of 30-fold. Sunlight contains high levels of NIR which likely stimulate mitochondrial melatonin production. High latitude has less NIR irradiation and excessive weight restricts NIR penetration to the important organs such as the lungs and heart. Thus, both obesity and high latitude are factors that limit local melatonin production and compromise the protective effects of locally-produced melatonin in these important organs. These observations may not only apply to COVID-19 patients but to other disorders including diabetes, neurodegenerative diseases and seasonal depression.
Published:
2022-10-03